During the treatment process, the dentist asks the question of how to fill the cavity, so the patient needs to know which fillings are best to put on the teeth, as well as the main advantages and disadvantages of certain materials in order to understand what he is paying money for.
The modern dental market offers a large number of various means for performing dental restorations. Some fillings are more suitable for front teeth, others - for molars, some have enhanced aesthetic qualities, others are characterized by enhanced strength properties. Let's look at the main types of filling materials used for making fillings.
Main types of fillings
There are two main types of dental restorations:
- permanent - the most extensive group of materials that are used to replenish the lost structure of enamel and dentin. Such fillings provide sealing, reliable closure of the prepared cavity, and depending on the type of substance used, they can prevent static caries, protect against relapses, or have increased aesthetics, due to which the restoration on the tooth will be invisible even upon close examination;
- temporary - applied in cases where delayed treatment over several visits is required in the treatment of pulpitis or periodontitis. A filling made of temporary material protects against the penetration of microorganisms and food particles into the root canal system. Due to the fact that substances used for this purpose have the ability to crumble or dissolve over time, they are installed for a period of no more than 10-14 days.
Materials
The means used to restore the anatomy of the tooth, its functions, appearance, as well as to prevent further destruction of hard tissues, have a clear classification, which is based on differences in the composition and properties of restoration materials.
- Cements are divided into mineral and polymer. The first group includes products based on phosphoric acid: silicate, silico-phosphate and zinc phosphate. Polymers are produced containing polyacrylic or other acids organic origin. These include polycarboxylate and glass ionomer cements.
- Plastics - can be filled (composite) or unfilled, produced on the basis of epoxy or acrylic resins.
- Composites are divided into chemical and light curing materials.
- Compomers are hybrids of composites and GIC.
- Metal materials for restorations - amalgams, gallium alloys and pure gold for direct filling.
Let's take a closer look at each of the groups.
Cement fillings
The most common group of dental materials used at budget appointments. Cements have the following advantages:
- high wear resistance;
- strength;
- prevention of recurrent caries due to the accumulation of fluoride from toothpastes and its gradual release;
- affordable price;
- easy to use;
- have a coefficient of thermal expansion close to that of dental tissues;
- good adhesion to dentin and enamel.
However this group materials have a number of significant disadvantages, which is why fillings made from them are not recommended to be placed in certain situations:
- sensitive to insufficient amount of liquid or its excess at the initial stage of hardening;
- low aesthetic properties;
- Difficulties in grinding and polishing the filling, which do not allow achieving a smooth, mirror-like surface of the restored part of the tooth.
Based on the listed qualities of cements, it is advisable to use them for restoration of molars, where resistance of the material to chewing loads is required, but aesthetic indicators are not critical.
Plastic
These fillings are also used at a free therapeutic appointment in dental clinics, however, they are less widespread in comparison with cements due to the specifics of working with them. In addition, such materials have other negative sides.
- Low resistance to mechanical pressure.
- Tendency to abrasion.
- Toxicity and bad smell when hardening.
- The fragility of restorations.
- High shrinkage rate of plastic during polymerization.
- Absorption of dyes from food and drinks.
Of the obvious advantages of the material, one can only highlight the similarity in external signs With hard tissues tooth, which is why plastic fillings are recommended to be placed on the front teeth, where there is no strong chewing load, but satisfactory appearance.
Chemical
Chemically cured composites are a two-component self-hardening system based on a polymer matrix. They are a more modern development in comparison with classic cement materials.
Due to the fact that the matrix of the chemically cured composite consists of an organic polymer resin and an inorganic filler introduced into it, the filling products of this group have unique properties in comparison with all previous representatives.
Advantages:
- uniform polymerization of the material, regardless of the thickness of the layer introduced into the cavity;
- satisfactory aesthetic data;
- good wear resistance;
- ease of finishing
- affordable price.
Flaws:
- a short work time material after mixing the components;
- excessive fluidity of some representatives of chemically cured composites;
- gray undertone in finished fillings due to the release of residual monomer;
- high shrinkage.
Despite many positive sides material, an increasing number of dentists are abandoning chemical composites in favor of photo-curing fillings.
Light
- no change physical qualities in the process of modeling a filling;
- there is no need to mix substances - photocomposites are presented as a homogeneous mass;
- the ability to combine different shades to obtain maximum resemblance to the natural color of the tooth;
- polymerization using a special lamp at the moment when the doctor needs it;
- waste-free use - the dentist takes as much material as he needs.
But, like any preparations for dental restoration, light composites have a number of negative qualities:
- long time for placing a filling due to the need for layer-by-layer application of the substance, no more than 2 mm thick, otherwise complete curing will not occur;
- high price;
- the light of the lamps used is harmful to the retina of the eye, for this reason it is necessary to work in protective glasses.
The materials are used for all types of dental restorations, as they have good strength, are well polished, are available in a wide palette of shades, and using a composite, you can create the natural anatomy of the tooth, taking into account the location of the cusps and fissures, which significantly increases the aesthetics of the fillings.
Amalgam
Metal fillings were widespread during the USSR, and in countries Western Europe are widely used at budget receptions to this day. And this is not surprising, because thanks to the presence of silver, the material has a caries-static effect, kills microorganisms, and is also the most durable of all the types of teeth filling products presented.
However, amalgams have limited use for several reasons.
- The mercury contained in the composition is toxic to the body.
- Dark gray color looks unattractive.
- There is no adhesion to the walls of the carious cavity.
- Stains dentin.
It is advisable to use such fillings only for restoration extensive defects chewing teeth.
Ceramic
Dental products made of porcelain are primary hard structures used to restore the integrity of the lost tooth structure. The most popular are ceramic inlays, which are not inferior to enamel in terms of resistance to mechanical stress. In addition, ceramics have high aesthetic values.
All designs made from this material have the following disadvantages:
- fragility;
- lack of adhesion to the tooth;
- it is necessary to use cements for fixation;
- high cost.
Compomer
Compomers are hybrid materials that, according to manufacturers, should have positive qualities light-curing composites and glass ionomer cements. Due to this, they have a high degree of similarity in appearance to hard tissues, are very durable, and resistant to chewing pressure. However, as shows clinical experience dentists, compomers:
- less aesthetically pleasing, durable and less polishable compared to photo composites;
- have less biocompatibility, worse caries-static effect and unsatisfactory adhesion.
For these reasons, the materials of the presented group have a limited scope.
Video: about dental fillings and types of filling material.
Additional questions
What fillings are best placed on chewing teeth?
It is necessary to install materials on the molars that can withstand high mechanical loads and do not wear off. Composites and GICs have these properties. Of the modern developments, ormokers – hybrids of photocomposites and ceramics – best satisfy the presented requirements.
Paid or free: which one to choose?
It is impossible to answer this question unequivocally, because the patient must make such a choice independently based on his financial situation. If a person has the ability to pay dental services, then it is better to choose paid fillings, since they use modern materials that make it possible to achieve maximum similarity with the color of the teeth, and also to fill the tooth so that there is no gap between the restoration and the dentin, into which microorganisms will subsequently penetrate, which will lead to recurrent caries .
Fillings for baby teeth
The most popular materials for restoring lost dental tissue in childhood are cements. The preparations allow you to quickly make a filling, adhere well to the tooth, and also release fluoride, which serves in a good way prevention of secondary caries. The Twinkie Star material, which belongs to the class of compomers, is popular among children, as it is available in several colors, and kids can choose a pink, golden or green filling according to their taste.
Dental fillings: what are they and why are they needed?
In dentistry, a filling is a material that is used to fill holes in teeth, which are usually formed during treatment, or when part of a tooth falls off on its own (hit, fell, and other mechanical options).
A dental filling is needed to isolate the sensitive tissues of our teeth in order to prevent microbes from getting here (the place where the hole or fracture has formed).
What types of dental fillings are there?
Dental fillings are divided into two types - temporary and permanent.
 Doctors most often place temporary fillings for some therapeutic or diagnostic purposes, for example, when the doctor is not entirely sure whether the dental nerve is damaged or not. In such cases, a temporary filling is placed: if the tooth begins to hurt while wearing such a filling, then there is a problem with the nerve and its removal is required.
Doctors most often place temporary fillings for some therapeutic or diagnostic purposes, for example, when the doctor is not entirely sure whether the dental nerve is damaged or not. In such cases, a temporary filling is placed: if the tooth begins to hurt while wearing such a filling, then there is a problem with the nerve and its removal is required.
Also, therapeutic fillings are often worn in various useful medicines, which need to be deleted after a certain amount of time. The temporary filling will not fall out on the 3rd day after the doctor installed it, it is simply much easier to remove it by the doctor who placed it. Such fillings are also placed when arsenic is covered.
Dentists have been placing permanent fillings for years and even decades.
Today, doctors have in their arsenal the following “building materials” for filling teeth.
Types of dental fillings:

Cement fillings come in several types. Most often, silicate cements, phosphate cements and glass ionomer cements are used for their production.
Silicate cement began to be used in the 19th century. The composition of the cement powder includes aluminosilicate glass, which, interacting with the liquid in the form of a mixture of phosphoric acids, forms a structured gel.
A positive property of this material is the release of fluoride ions, which helps to avoid secondary caries. The disadvantage of the filling is the fact that silicate cement releases free phosphoric acid, which negatively affects the living pulp. Therefore, it is not recommended to install these cements without a liner.
Fillings made of silicate cement allow you to choose different shades.
Phosphate cements are a cheap material that has weak fixation, wears off quickly and does not adhere well to the edges of the tooth, which leads to the penetration of microbes. Therefore, in order to strengthen the strength of such a filling, various fillers (most often silver) are added to the cement.
Unlike phosphate cements, glass ionomer cements are chemical properties similar to tooth tissues. Hardening of these fillings occurs under the influence of ultraviolet radiation, which gives the doctor time to slowly make the filling while it is soft, and only then “harden” it.
Thanks to components containing fluoride, such a filling will help avoid secondary caries; they are more durable. However, glass ionomer cements also have rapid abrasion and brittleness, and the addition of food coloring for coloring does not make the tooth look natural.
 Metal fillings are made from amalgam (silver amalgam consists of apillar containing 60% silver, 20% copper, 4-5% others (tin, silicon, etc.) with mercury). Despite the strength, durability and low cost, modern dentistry is used less and less.
Metal fillings are made from amalgam (silver amalgam consists of apillar containing 60% silver, 20% copper, 4-5% others (tin, silicon, etc.) with mercury). Despite the strength, durability and low cost, modern dentistry is used less and less.
Metal fillings have a shiny color that contrasts sharply with the tooth enamel. It is acceptable to place an amalgam filling only on the back teeth, while maintaining the thick walls of the tooth.
Contraindications: presence of a metal structure in the oral cavity (to avoid galvanism); upon receipt by the patient radiation therapy V maxillofacial area; filling of anterior (front) teeth.
 Composite plastics are plastic masses the color of tooth enamel with a glass filler (silicon dioxide). Introduced in 1960, they were used exclusively on the front teeth, because their strength did not allow them to withstand the loads experienced by chewing teeth.
Composite plastics are plastic masses the color of tooth enamel with a glass filler (silicon dioxide). Introduced in 1960, they were used exclusively on the front teeth, because their strength did not allow them to withstand the loads experienced by chewing teeth.
Since that time, composite materials have improved so much that they can now be used on chewing teeth. Composite materials are used not only to restore teeth after caries, but also for cosmetic purposes to change the color of a tooth or its shape.
How is a composite filling placed?
After preparing the tooth, the filling is placed in layers with each layer highlighted. After the process is completed, the dentist grinds the composite filling according to the shape of the tooth. The filling is then polished to extend its life.
How long does it take to place a composite filling?
It takes 20 minutes longer than an amalgam filling. The duration of the procedure is affected by the size of the filling and its location in the oral cavity. The larger the filling, the longer it takes.
What is the cost of such a filling?
The price may vary, but usually it is 1.5-2 times higher than amalgam fillings. Most insurance companies cover the cost of composite fillings up to the cost of amalgam fillings, leaving the rest to the patient.
But, as composite materials are constantly being improved, the likelihood of more complete reimbursement of the costs of composite fillings increases.
What are the advantages of composite fillings?
After installation of a composite filling, the patient may experience increased sensitivity. The color of the filling may change slightly if the patient drinks tea, coffee or other caustic drinks. The doctor may cover the filling with a transparent film to avoid discoloration if this aspect is important to the patient. Composite materials tend to wear out faster on larger fillings compared to amalgam fillings.
How long does a composite filling last?
Studies have shown that, on average, a composite filling lasts 7-10 years, while the service life of an amalgam filling is slightly longer.
 Compomer material used for filling small cavities, wedge-shaped defects, baby teeth, restoration of teeth that do not bear a large chewing load and creation of inlays. It combines the strength of composite fillings, protection against caries, like glass ionomers, and good aesthetic properties.
Compomer material used for filling small cavities, wedge-shaped defects, baby teeth, restoration of teeth that do not bear a large chewing load and creation of inlays. It combines the strength of composite fillings, protection against caries, like glass ionomers, and good aesthetic properties.
Compomer inlays are used in cases of severe tooth decay, when virtually only the walls remain. The inlay is made from an impression in a dental laboratory and then glued into the tooth. Such fillings are more expensive, but they are durable and aesthetically pleasing.
 An inlay is, surprisingly, also a filling, only made not in the patient’s mouth, but in a laboratory. Even a composite inlay made from conventional filling material is free from the disadvantages described above that are inherent in a filling made in the mouth. If we talk about a ceramic inlay, it generally significantly surpasses any other in its properties.
An inlay is, surprisingly, also a filling, only made not in the patient’s mouth, but in a laboratory. Even a composite inlay made from conventional filling material is free from the disadvantages described above that are inherent in a filling made in the mouth. If we talk about a ceramic inlay, it generally significantly surpasses any other in its properties.
The fact is that of all the materials used in dentistry, ceramics are closest in their properties (strength, light reflection, etc.) to tooth enamel. A porcelain inlay glued to the tooth almost completely restores its strength. Therefore, where there is extensive tooth decay, it is preferable to place an inlay rather than a filling.
In many cases, when the destruction of the coronal part of the tooth is great, and the tooth is still alive, the only thing that allows you to avoid depulping and covering the tooth with a crown is an inlay.
The impetus for the development of this technology was the improvement of the mechanism for gluing (or adhesion) of fillings to the tooth. If previously fillings were held in the cavity due to their geometry, now doctors have begun to create microscopic irregularities in the enamel, into which the glue that connects the filling to the tooth flows.
Today, dental adhesives (they are called adhesive systems) of the fourth and fifth generations penetrate micropores in all layers of the tooth, both enamel and dentin.
Penetrating into all the microscopic irregularities, of which there are a huge number, the glue (adhesive) creates such a connection between the filling and the tooth that in an experiment, when trying to tear off the filling, it comes off along with part of the tooth. Thanks to the creation of dental miracle glues (adhesives), it became possible to glue not only composite fillings to teeth, but also porcelain, metal, and many other materials.
 Human factor
Human factor
Of course, the role of the doctor in dental treatment is undeniable. Without him it is simply impossible to do this. And the doctor is also not insured against mistakes due to his inattention or dishonesty, lack of time or desire to do everything correctly, or perhaps due to ignorance (surprisingly, this also often occurs).
The main possible reasons for the rapid loss of a filling from a tooth:
- Insufficient cleansing of the carious cavity from affected tissues. Simply put, when a doctor leaves decay in a cavity and “seals” it under a filling. Only the process of tooth destruction continues and, as a result, a decrease in the strength of attachment of the filling to the walls and bottom of the formed cavity, a disruption of the connection between the material and tooth tissue.
- Incorrectly formed cavity for filling. There are specific rules for each case of the location of the carious lesion. According to Black's classification, carious cavities are not only divided depending on their location, but also the principle of formation of each of them is clearly defined. And these rules must be followed.
- Many materials used for filling teeth are very sensitive to moisture and when saliva gets into the prepared cavity, they greatly reduce the chances of the filling lasting a long time. This is relevant when treating baby teeth in children, as well as in cases of limited mouth opening, profuse salivation in the patient or the location of the carious cavity near the gum edge.
- Light-curing filling materials harden after being introduced into the prepared cavity only under the influence of light of a certain wavelength (450-500 nm). For this purpose, dental polymerization lamps are used, powered either by a battery or from a dental unit. It is important to monitor the battery charge level, otherwise the depth of light penetration and its strength are sharply reduced. The filling can only harden on the outside, while the inner layers will remain soft. This means that such a filling will soon fall out of the cavity.
![]() The dentist has a large selection of materials with different properties in his arsenal. They can be chemically cured (the filling becomes hard when two pastes are mixed for several minutes or hours), light-cured (hardens immediately when illuminated).
The dentist has a large selection of materials with different properties in his arsenal. They can be chemically cured (the filling becomes hard when two pastes are mixed for several minutes or hours), light-cured (hardens immediately when illuminated).
There are also materials for temporary fillings that harden in the mouth under the influence of body temperature and saliva moisture over several hours.
This means that the recommendations that the doctor gives to the patient depend on what the filling is made of. For example, not eating or chewing gum for 2 hours.
There is another characteristic of materials - shrinkage, i.e. a decrease in volume of the filling over time. This indicator varies greatly for different materials. When placing a filling, the doctor takes into account the degree of possible shrinkage of the material, reducing the risk of cracks, the appearance of the filling-tooth boundary, or its loss.
By the way, this mechanism explains the fact that over time such a border becomes noticeable even to the patient; it becomes stained with plaque and turns yellow. filling in in this case better to change it. If this is not done, then it is in this place that, as a rule, secondary (recurrent) caries begins around the fillings.
 Individual structural features of enamel and dentin:
Individual structural features of enamel and dentin:
The tissues from which teeth are formed are formed as early as the 7th week. intrauterine development, this moment can be considered the beginning of their development. Depending on the impact of adverse factors on the body expectant mother or child (at the time of formation permanent teeth), the strength of enamel and dentin will be different.
Toxicoses of a pregnant woman, lack of calcium, fluorine and other elements, viral infections and medications taken greatly affect the development of teeth in a child. Likewise, at the stage of formation of permanent teeth, many factors affect the future features of the structure of dental tissues.
For example, when fluoride enters the body in excess, the enamel does not develop properly. The mechanism of action of fluoride is based on the fact that it is integrated into the structure of hydroxyapatite crystals (the main building element of enamel), replacing calcium, as a result of which areas of such enamel become less dense and more fragile, and change color.
Distinct white spots are visible on the teeth; the enamel of such teeth is prone to chipping; fillings do not hold well due to the disruption of the enamel structure. The structure of enamel can change with the development of hypoplasia, disruption of amelo- and dentinogenesis (formation of enamel and dentin), and hereditary diseases.
The thickness of the tooth tissue also matters. With pathological abrasion, this indicator decreases, and after placing a filling, the process does not stop at all, reducing over time the degree of fixation of the material to the tooth.

Dental materials for filling temporary teeth must meet many requirements. One of the main ones is non-toxicity and safety for children. Due to lack chemical exposure On dental tissue, such materials are fixed in the cavity only due to mechanical adhesion forces.
Simply put, they are connected like puzzle elements, matching each other in shape and size. There is no chemical bond. And such materials harden within 1-2 hours, remaining sensitive to moisture, which makes the filling vulnerable during this time.
Such fillings wear out over time and shrink in volume. Yes, and in principle the difficulty of treatment baby tooth in a child is obvious to everyone (it is difficult to create ideal conditions for a doctor to work).

Let's return to the properties of materials for fillings. If they do not harden immediately, but some time after being placed in the tooth, then the doctor gives clear recommendations to the patient. For example, do not eat for 2 hours and do not chew gum. But the patient is not always so obedient, especially a small child.
For adults important factors, allowing to extend the durability of the filling are:
- oral hygiene (bacteria live and actively multiply in dental plaque, softening the enamel due to the acids produced)
- quality of nutrition (aggressive foods that destroy enamel, reduce the degree of fixation of fillings). This includes soda, products with various acids, sweets, flour products, sharp changes food temperatures from cold to hot and vice versa. The lack of calcium in the body also plays a role, which compensates for bone and tooth enamel.
- bad habits (for example, frequent consumption of seeds, crackers, nuts leads to the appearance of microcracks in the enamel structure, which gradually deepen, causing either chips of the enamel or loss of the filling).
Timely treatment of caries determines not only success in preserving healthy teeth, but also prevents the loss of already placed fillings.
You need to take care of your teeth on time and not wait until toothache will remind you of their existence. Putting a filling is only half the battle. How long it stays in the tooth depends not only on the doctor and his professional qualities, but also from the patient himself.
Lifestyle modern man cannot be called healthy. Not proper nutrition, regular stress and anxiety, smoking abuse - all this leads to the development various diseases. And first of all, our teeth suffer.
Their treatment is an unpleasant process, but necessary. Sometimes it is enough to take a complex preventive measures, but quite often patients are recommended to have a tooth filled. It is this procedure that we will talk about in the article.
Tooth filling process
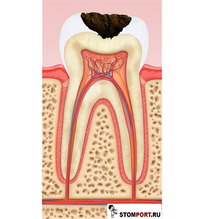
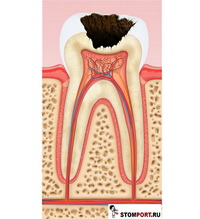
Tooth filling is indicated when caries penetrates beyond the enamel layer. If a filling is not placed in time, the tooth will gradually deteriorate, which will lead to the formation of a hole and the occurrence of pulpitis. This process is always accompanied by acute pain.
How is a diseased tooth treated? If caries has led to the development of pulpitis, the dentist first removes the nerve with all its smallest processes, then fills the root canal and the tooth itself. The nerve can be saved in the case when caries has just made itself known - it is enough to restore the enamel using a special solution.
When filling a filling, the dentist first removes the diseased tissue and then thoroughly cleans the infected area. Only after this the hole is filled with a filling. It prevents further development caries, and consequently tooth decay.
Types of fillings
When filling a tooth Special attention should be given to choosing the type of filling. There are the following varieties of it, differing in quality and cost:
- An amalgam filling is a durable alloy of metal and mercury. It is durable, does not shrink and is resistant to moisture. Despite such great advantages, this filling is used very rarely because it is not aesthetically pleasing and toxic.
- Phosphate cements are the cheapest type of filling. Nowadays it is not popular due to its fragility and toxicity. In addition, it is very difficult to choose a filling that matches the color of the tooth. Today, in the vast majority of cases, phosphate cements are used to fill children's primary teeth.
- Glass ionomer cements are widely used in both pediatric and adult dentistry. Unlike phosphate cements, they are absolutely non-toxic and resistant to moisture. In addition, these fillings contain fluoride ions, which help strengthen tooth tissue. Despite all their advantages, they are not the most popular. Glass ionomer cements wear out very quickly and do not have sufficient aesthetics.
- Composite fillings are divided into two main groups - chemical curing and light curing. The former are highly durable, but at the same time somewhat toxic and darken over time. The latter are aesthetic, durable and non-toxic. However, they also have a significant drawback - they have a high shrinkage coefficient. It is worth noting that there are three types of light-curing fillings - microfilled, macrofilled and hybrid. They differ in strength.
- Compomers are fillings that combine the properties of glass ionomer cement and a hybrid composite. They are the most popular due to their high strength, aesthetics, and non-toxicity.
The choice of filling depends on many factors - the degree of damage, its location, the financial capabilities of the patient and others. In any case, this should only be done by a specialist who fills the tooth.
Filling is a popular dental procedure. Filling - filling the dental cavity with a special composition. Filling materials are varied, but light filling is considered the most modern and high-quality. It has many names: photopolymer, reflective, polymer, light-hardening, etc. Unlike chemical fillings, light-curing ones are invisible, so they are better suited for front teeth. A photopolymer filling will not only last for many years, but will also preserve the beauty of your smile.
Concept of light seal
The material from which light fillings are made hardens when exposed to ultraviolet light. A permanent photo seal has a number of advantages. The most important advantage is considered to be a wide palette of colors, thanks to which it is almost impossible to notice the filled area if the filling is placed correctly.
Compound
The main component of the light filling, to which it owes its properties and name, is heliocomposite. When exposed to light, it breaks down into radicals, which leads to polymerization of the light filling.
In addition to heliocomposite, the gel filling contains fillers that affect its appearance and quality. The service life depends on them.
Macrophiles are large inorganic elements. They give the following properties:

Microphiles are small particles that impart properties such as:
- light polishing;
- glossy shine;
- color stability;
- instability to mechanical loads.
Mini-fillers combine the properties of previous particles, but are rarely used. They are suitable for restoring teeth with minor defects, as they have:
- average resistance to mechanical damage;
- difficulty in polishing;
- low strength.
Nanohybrid composites are ultrafine particles that combine the best properties. Such fillings are suitable for restoring teeth of varying degrees of damage. Once placed, the filling is completely invisible.
What does a photofill look like: photos before and after treatment
 The dentist selects the material and color of the light filling that is closest to the natural shade of the enamel. Much depends on the qualifications of the doctor - if he does the job efficiently (without cracks, chips, etc.), then the restored tooth will be invisible. The last thing on which the condition of the light-polymer filling depends is oral care.
The dentist selects the material and color of the light filling that is closest to the natural shade of the enamel. Much depends on the qualifications of the doctor - if he does the job efficiently (without cracks, chips, etc.), then the restored tooth will be invisible. The last thing on which the condition of the light-polymer filling depends is oral care.
If certain rules are followed, the design will retain its original appearance. In the photo you can see what it looks like oral cavity before and after placing a filling.
When is use indicated?
Permanent fillings are used to eliminate many defects, not necessarily carious ones. Indications for installing a light seal are:
- carious cavities on the entire surface of the tooth crown;
- destruction of the tooth crown up to ½ part of its volume;
- defects in the root or neck of the tooth;
- pigmentation that cannot be removed by other means;
- defects not associated with caries.
What types of light fillings are there?
 Light polymer fillings differ in their purpose. They can be installed on the front or chewing teeth. For the front teeth, higher quality materials containing microfils are selected, since they are not visible during a conversation, smile, etc. For others, macrophiles are suitable, which are inferior to fine particles in aesthetic terms, but have advantages in strength.
Light polymer fillings differ in their purpose. They can be installed on the front or chewing teeth. For the front teeth, higher quality materials containing microfils are selected, since they are not visible during a conversation, smile, etc. For others, macrophiles are suitable, which are inferior to fine particles in aesthetic terms, but have advantages in strength.
A type of light seal that can be called universal - containing ultra-fine particles. They fill any dental defects.
On the anterior (front) teeth
Treatment of anterior teeth with a composite stands out separately, since not only strength is important, but also appearance. For this reason, a higher quality material is used for photopolymer fillings; it contains micro-filled particles. Thanks to them, it becomes possible to choose the perfect color (and save it for for a long time), they also have a shine characteristic of enamel.
On chewing teeth
Resistance to mechanical damage is important for chewing teeth, since they bear the entire load during chewing food. Photopolymer fillings for chewing teeth contain macro-filled particles that provide strength and wear resistance.
The downside is the unstable color, but for this type of teeth aesthetics are less important than treatment. In any case, a light filling is less noticeable than a chemical, glass ionomer, etc.
Installation process and service life
The process of installing a light filling differs little from other types of filling. Tooth filling consists of several stages:
- Examination of the oral cavity and application of local anesthesia.
- Removal of carious area.
- Choice of shade. The dentist uses a special scale. This filling stage can be carried out before the procedure begins.
- Preparing for tooth filling. It is isolated with cotton swabs, and a saliva ejector is installed to prevent saliva from entering.
- Drying the treated area. After this, it is coated for 40 seconds with a special preparation that loosens dentin for better adhesion of the filling to the tooth. Then it is washed off and the surface is dried again.
- Application of adhesive. It enhances adhesion to dentin.
- Formation. The material is applied in stages, in layers. Each layer is exposed to ultraviolet light for 1-2 minutes.
- Grinding to create shape, correct bite, etc.
- Coating the tooth surface with a protective fluoride varnish. It strengthens the enamel and additionally secures the filling in the crown of the tooth.
All stages of filling last from half an hour to an hour and are not accompanied by pain. A photo seal can last from three to five years.
How long after can I eat?
After installing any type of filling, you must follow the dentist's recommendations. The light seal is no exception. Usually everyone is concerned about the first meal after installation. You can eat in 40 minutes, but to be on the safe side, it is advisable to wait 2 hours. These precautions will extend the life of the tooth filling.
For the first few days, it is advisable not to eat foods containing aggressive pigments. You will have to abstain a little from pomegranate, cherry juice, tea, coffee, borscht, beets and other things. This will maintain the shade of the filling so that it does not differ from other teeth in color.
Sweets and flour products are also prohibited. These products create a favorable environment for the proliferation of bacteria and other microorganisms.
How is it different from other types of filling?
To talk about how light-polymer filling materials differ from others, you need to understand what they are like:

 We can say that a photopolymer filling is the best, as it combines the advantages of all others without any significant disadvantages. It is non-toxic, like cement (even pregnant women are allowed to install it), is invisible, which distinguishes it from chemical ones, and therefore is suitable for filling front teeth. The light-curing composite is plastic, so it is more convenient to install (everything is done easier, since it is easy to grind), it can be used independently, unlike glass ionomer material. The only disadvantage of a gel filling is that its use is justified only as a permanent filling due to its high price.
We can say that a photopolymer filling is the best, as it combines the advantages of all others without any significant disadvantages. It is non-toxic, like cement (even pregnant women are allowed to install it), is invisible, which distinguishes it from chemical ones, and therefore is suitable for filling front teeth. The light-curing composite is plastic, so it is more convenient to install (everything is done easier, since it is easy to grind), it can be used independently, unlike glass ionomer material. The only disadvantage of a gel filling is that its use is justified only as a permanent filling due to its high price.
Service life of light seals
The service life of a light filling, if the dentist’s recommendations are followed, is 5-6 years. You should maintain oral hygiene, go for regular checkups, brush your teeth twice a day, etc.
Nutrition matters. It is advisable to monitor it not only in the first week after the filling is placed. This does not mean that it is necessary to switch to a strict healthy diet, excluding sweets, flour, fatty and other foods from the diet.
You can increase the amount of vegetables, fruits, and dairy products in your diet and stick to a normal diet, eliminating daily trips to fast foods, excessive consumption of processed foods, etc. Most people eat this way, there is nothing special about it.
As you know, the most common materials for filling teeth are light-curing composites. Taking this fact into account, let’s consider the technology for installing a photocomposite filling.
The method of filling a tooth directly depends on the volume and depth of the carious process. Based on the depth of the carious cavity, caries is classified as: superficial, medium and deep. At superficial caries, the carious defect is located within the enamel. In moderate cases, the enamel is affected and the dentin is affected. At deep caries– the enamel is damaged and a significant layer of dentin is destroyed by caries.
Superficial caries
Average caries
Deep caries
After the carious cavity is prepared for filling, the tooth must be isolated from saliva. Failure to comply with this requirement can lead to wetting of the prepared cavity with saliva and, as a result, cause a violation of the tightness of the filling to the tooth. This leads to caries at the border of the filling and the tooth, and can also cause “fallout”.
To isolate teeth from saliva, use cotton swabs or more reliable way– insulation using rubber dam. A rubber dam (or rubber dam) is a thin sheet of latex rubber. Special reception a sheet of rubber dam is placed on the tooth, creating a dry working field. Saliva is removed from the mouth using a saliva ejector.
Figure 1: Rubber dam sheet.

Fig. 2: Clasps - metal clips for fixing the rubber dam to the tooth.

Figure 3: Tooth isolated with rubber dam.

Then acid etching of the prepared cavity is carried out using 37% phosphoric acid. This is done in order to remove the so-called “smear layer” and increase the contact area between the surface of the tooth cavity and the filling. During etching, the acid dissolves the inorganic components of the tooth tissue, creating a rough surface. After 20–60 seconds, the acid is washed off with water and the tooth is dried with air.
The next step is to introduce the so-called “bond” into the cavity - its function is to create an “adhesive” layer for reliable “adhesion” of the filling to the tooth tissue.
Applying bond to the walls of the prepared cavity

After bonding, the walls of the cavity are covered with a special special flowable composite. Thanks to its fluidity, it penetrates into all microcavities, creating a thin and smooth “adaptive” layer. This layer helps relieve mechanical stress from the walls of the tooth cavity. Then the flowable composite introduced into the cavity is cured with the light of a special dental lamp.
Dental curing lamp

Light curing of fillings

The filling material is directly introduced into the cavity in portions and evenly distributed in it. After which it is cured with lamp light. So, layer by layer, the entire cavity is filled. It is very important that the thickness of each layer does not exceed 2 mm. This requirement is associated with polymerization shrinkage of the photocomposite (reduction in volume during curing) and the inability to polymerize a “thick” layer of the composite with lamp light. If this rule is not followed, a microgap may form between the filling and the tooth tissue, which leads to recurrent caries. This mistake can also cause pain after the filling is placed.
So, “set.” Now it should be processed, i.e. give the restored tooth the correct anatomical shape and polish the filling. Pre-treatment of the filling is carried out using diamond or carbide burs. Excess filling material is removed, sharp edges are smoothed, and the filling is given a relief characteristic of a given tooth. To control the full contact between the restored tooth and the antagonist (a similar tooth in the opposite jaw), carbon paper is used. When the teeth are closed, the paper leaves an imprint on the filling in the place where the contact is excessive. This point is sanded. This operation is repeated until optimal contact between the antagonists is achieved. For final processing of the filling, polishing rubber bands, abrasive discs and strips are used. After which the filling is polished with a special polishing paste and coated with a protective varnish.
Clinical example of heliocomposite
A: Initial situation (amalgam fillings requiring replacement).

B: The fillings are removed and the resulting cavities are etched and covered with bonding agent.

C, D, E: Stages of restoration of the second upper premolar.




F, G, H: Stages of restoration of the first upper molar. 
View of the completed dental restoration.
Features of the treatment of medium and deep caries
With moderate and, especially, deep caries, the layer of tooth tissue separating the bottom of the carious cavity from the pulp chamber (the inner part of the tooth where the “nerve” is located) can be very thin. As a result, after placing a filling, a complication may occur - (inflammation of the nerve of the tooth). Pulpitis, in this case, can be provoked by chemical irritation of the pulp by dental preparations used to treat the carious cavity.
Also, a significant area of exposed (internal tooth tissue containing nerve endings) can cause pain after tooth filling. In order to prevent these undesirable consequences, before placing the filling, the inner surface of the prepared cavity is covered with a thin layer of glass ionomer cement. The cement layer promotes the regeneration of tooth tissue and isolates sensitive dentin from the irritating effect of the etchant acid.
In case of deep caries, a special therapeutic pad is applied to the bottom of the cavity. It contains calcium hydroxide, which helps restore dentin from the pulp chamber. Then a layer of glass ionomer cement is applied over the treatment pad, after which a filling is placed.
A “good” filling will be obtained if the above principles of caries treatment are observed. In other cases, the filling will most likely not be “good” enough.

 Echo HSG tubal patency")





