Human teeth are integral part chewing-speech apparatus, which, according to modern views, is a complex of interacting and interconnected organs that take part in chewing, breathing, and the formation of voice and speech. This complex includes: solid support - the facial skeleton and the temporomandibular joint; masticatory muscles; organs designed for grasping, moving food and forming a bolus of food, for swallowing, as well as the sound-speech apparatus: lips, cheeks, palate, teeth, tongue; organs for crushing and grinding food - teeth; organs serving for softening and enzymatic processing of food - salivary glands oral cavity.
Teeth are surrounded by various anatomical structures. They form metameric dentition on the jaws, so the area of the jaw with the tooth belonging to it is designated as dentofacial segment. Dentofacial segments are distinguished upper jaw(segmenta dentomaxillares) and lower jaw (segmenta dentomandibularis).
The dentofacial segment includes the tooth; the dental alveolus and the part of the jaw adjacent to it, covered with mucous membrane; ligamentous apparatus, fixing the tooth to the alveolus; vessels and nerves (Fig. 1).
Rice. 1.
1 - periodontal fibers; 2 - alveolar wall; 3 - dentoalveolar fibers; 4 - alveolar-gingival branch of the nerve; 5 - periodontal vessels; 6 - arteries and veins of the jaw; 7 - dental branch of the nerve; 8 - bottom of the alveoli; 9 - tooth root; 10 - neck of the tooth; 11 — tooth crown
Human teeth belong to the heterodont and thecodont systems, to the diphyodont type. First, milk teeth (dentes decidui) function, which appear completely (20 teeth) by the age of 2 years, and then are replaced permanent teeth(dentes permanents) (32 teeth) (Fig. 2).

Rice. 2.
a - upper jaw; b - lower jaw;
1 - central incisors; 2 - lateral incisors; 3 - fangs; 4 - first premolars; 5 - second premolars; 6 - first molars; 7 - second molars; 8 - third molars
Parts of a tooth. Each tooth (dens) consists of a crown (corona dentis) - a thickened part protruding from the jaw alveolus; neck (cervix dentis) - the narrowed part adjacent to the crown, and root (radix dentis) - the part of the tooth lying inside the alveolus of the jaw. The root ends apex of tooth root(apex radicis dentis) (Fig. 3). Functionally different teeth have an unequal number of roots - from 1 to 3.
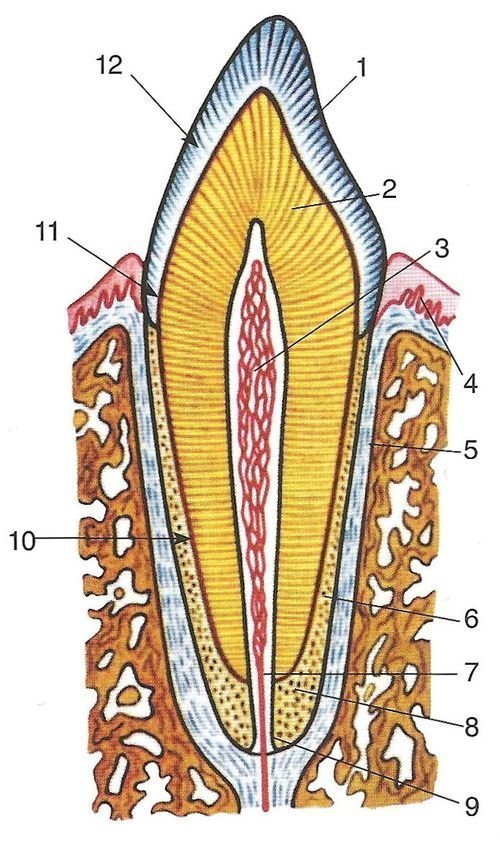
Rice. 3. Tooth structure: 1 - enamel; 2 - dentin; 3 - pulp; 4 - free part of the gum; 5 - periodontium; 6 - cement; 7 - tooth root canal; 8 - alveolar wall; 9 — hole in the apex of the tooth; 10 - tooth root; 11 - neck of the tooth; 12 — tooth crown
In dentistry there are clinical crown(corona clinic), which is understood as the area of the tooth protruding above the gum, as well as clinical root(radix clinic)- the area of the tooth located in the alveolus. Clinical crown with age, due to gum atrophy, it increases, and the clinical root decreases.
Inside the tooth there is a small dental cavity (cavitas dentis), the shape of which is different in different teeth. In the crown of a tooth, the shape of its cavity (cavitas coronae) almost repeats the shape of the crown. Then it continues to the root in the form root canal (canalis radicis dentis), which ends at the tip of the root hole (foramen apices dentis). In teeth with 2 and 3 roots there are, respectively, 2 or 3 root canals and apical foramina, but the canals can branch, bifurcate and reconnect into one. The wall of the tooth cavity adjacent to its closure surface is called the vault. In small and large molars, on the occlusal surface of which there are chewing tubercles, corresponding depressions filled with pulp horns are noticeable in the vault. The surface of the cavity from which the root canals begin is called the floor of the cavity. In single-rooted teeth, the bottom of the cavity narrows funnel-shaped and passes into the canal. In multi-rooted teeth, the bottom is flatter and has holes for each root.
The tooth cavity is filled pulp of the tooth (pulpa dentis)- loose connective tissue of a special structure, rich in cellular elements, vessels and nerves. According to the parts of the tooth cavity, they are distinguished crown pulp (pulpa coronalis) And root pulp (pulpa radicularis).
General tooth structure. The hard base of the tooth is dentin- a substance similar in structure to bone. Dentin determines the shape of the tooth. The dentin that forms the crown is covered with a layer of white dental enamel (enamelum), and root dentin - cement (cementum). The junction of the crown enamel and root cement is at the neck of the tooth. There are 3 types of connection between enamel and cement:
1) they are connected end-to-end;
2) they overlap each other (enamel overlaps cement and vice versa);
3) the enamel does not reach the edge of the cement and an open area of dentin remains between them.
The enamel of intact teeth is covered with a durable, lime-free cuticle enamel (cuticula enameli).
Dentin is the primary tissue of teeth. Its structure is similar to coarse-fibered bone and differs from it in the absence of cells and greater hardness. Dentin consists of cell processes - odontoblasts, which are located in the peripheral layer of the tooth pulp, and the surrounding main substance. It contains a lot dentinal tubules (tubuli dentinales), in which the processes of odontoblasts pass (Fig. 4). In 1 mm 3 of dentin there are up to 75,000 dentinal tubules. In the dentin of the crown near the pulp there are more tubes than in the root. The number of dentinal tubules varies in different teeth: in incisors there are 1.5 times more of them than in molars.

Rice. 4. Odontoblasts and their processes in dentin:
1 - mantle dentin; 2 - peripulpar dentin; 3 - predentin; 4 - odontoblasts; 5 - dentinal tubules
The main substance of dentin, lying between the tubules, consists of collagen fibers and their adhesive substance. There are 2 layers of dentin: outer - mantle and inner - peripulpar. In the outer layer, the fibers of the main substance run at the top of the tooth crown in the radial direction, and in the inner layer - tangentially with respect to the tooth cavity. In the lateral sections of the crown and in the root, the fibers of the outer layer are located obliquely. In relation to the dentinal tubules, the collagen fibers of the outer layer run parallel, and the inner layer runs at a right angle. Mineral salts (mainly calcium phosphate, calcium carbonate, magnesium, sodium and hydroxyapatite crystals) are deposited between the collagen fibers. Calcification of collagen fibers does not occur. Salt crystals are oriented along the fibers. There are areas of dentin with slightly calcified or completely uncalcified ground substance ( interglobular spaces). These areas can increase during pathological processes. In older people, there are areas of dentin in which the fibers are also susceptible to calcification. Most inner layer peripulpal dentin is not calcified and is called dentinogenic zone (predentin). This zone is the place constant growth of dentin.
Currently, clinicians distinguish the morphofunctional formation endodontium, which includes pulp and dentin adjacent to the tooth cavity. These dental tissues are often involved in local pathological process, which led to the formation of endodontics as a section therapeutic dentistry and development of endodontic instruments.
The enamel consists of enamel prisms (prismae enameli)- thin (3-6 microns) elongated formations, running in waves through the entire thickness of the enamel, and gluing them together interprismatic substance.
The thickness of the enamel layer varies in different parts of the teeth and ranges from 0.01 mm (at the neck of the tooth) to 1.7 mm (at the level of the chewing cusps of the molars). Enamel is the hardest tissue of the human body, which is explained by its high (up to 97%) content of mineral salts. Enamel prisms have a polygonal shape and are located radially to the dentin and longitudinal axis tooth (Fig. 5).
Rice. 5. The structure of the human tooth. Histological specimen. Uv. x5.
Odontoblasts and their processes in dentin:
1 - enamel; 2 - oblique dark lines - enamel stripes (Retzius stripes); 3 — alternating enamel stripes (Schreger stripes); 4 - tooth crown; 5 - dentin; 6 - dentinal tubules; 7 - neck of the tooth; 8 - tooth cavity; 9 - dentin; 10 - tooth root; 11 - cement; 12 - tooth root canal
Cementum is coarse fibrous bone, consisting of main substance, impregnated with lime salts (up to 70%), in which collagen fibers run in different directions. The cement on the root tips and on the interroot surfaces contains cells - cementocytes, lying in the bone cavities. There are no tubes or vessels in the cement; it is nourished diffusely from the periodontium.
The root of the tooth is attached to the alveolus of the jaw through many bundles of connective tissue fibers. These bunches are loose connective tissue and cellular elements form the connective tissue membrane of the tooth, which is located between the alveolus and cement and is called periodontium. The periodontium plays the role of the internal periosteum. This attachment is one of the types of fibrous connection - dentoalveolar connection (articulation dentoalveolaris). The set of formations surrounding the tooth root: periodontium, alveolus, the corresponding section of the alveolar process and the gum covering it is called periodontal (parodentium).
The tooth is fixed using periodontal tissue, the fibers of which are stretched between the cement and the bone alveolus. The combination of three elements (bone dental alveolus, periodontium and cementum) is called supporting apparatus of the tooth.
The periodontium is a complex of connective tissue bundles located between the bone alveoli and cement. The width of the periodontal gap in human teeth is 0.15-0.35 mm near the mouth of the alveolus, 0.1-0.3 mm in the middle third of the root, and 0.3-0.55 mm at the root apex. In the middle third of the root, the leriodontal gap has a constriction, so it can be roughly compared in shape to hourglass, which is associated with micromovements of the tooth in the alveolus. After 55-60 years, the periodontal fissure narrows (in 72% of cases).
Many bundles of collagen fibers extend from the wall of the dental alveoli to the cementum. In the spaces between the bundles of fibrous tissue there are layers of loose connective tissue in which cellular elements (histiocytes, fibroblasts, osteoblasts, etc.), vessels and nerves lie. The direction of bundles of periodontal collagen fibers is different in various departments. At the mouth of the dental alveolus (marginal periodontium) in the retaining apparatus, one can distinguish dentogingival, interdental and dentoalveolar group bundles of fibers (Fig. 6).

Rice. 6. Structure of the periodontium. Cross section at the level of the cervical part of the tooth root: 1 - dentoalveolar fibers; 2 - interdental (interroot) fibers; 3 - periodontal fibers
Dental fibers (fibrae dentogingivales) begin from the root cement at the bottom of the gingival pocket and spread fan-shaped outward into the connective tissue of the gums.
The bundles are well expressed on the vestibular and oral surfaces and relatively weakly on the contact surfaces of the teeth. The thickness of the fiber bundles does not exceed 0.1 mm.
Interdental fibers (fibrae interdentaliae) form powerful beams 1.0-1.5 mm wide. They extend from the cementum of the contact surface of one tooth through the interdental septum to the cementum of the adjacent tube. This group of bundles plays a special role: it maintains the continuity of the dentition and participates in the distribution of chewing pressure within the dental arch.
Dentoalveolar fibers (fibrae dentoalveolares) start from the cementum of the root along the entire length and go to the wall of the dental alveoli. Bundles of fibers begin at the apex of the root, spread almost vertically, in the apical part - horizontally, in the middle and upper thirds of the root they go obliquely from bottom to top. On multi-rooted teeth, the bundles go less obliquely; in places where the root is divided, they follow from top to bottom, from one root to another, crossing each other. In the absence of an antagonist tooth, the direction of the beams becomes horizontal.
The orientation of bundles of periodontal collagen fibers, as well as the structure of the spongy substance of the jaws, are formed under the influence of functional load. In teeth devoid of antagonists, over time, the number and thickness of periodontal bundles become smaller, and their direction turns from oblique to horizontal and even oblique in the opposite direction (Fig. 7).

Rice. 7. Direction and severity of periodontal bundles in the presence (a) and absence of an antagonist (b)
Human anatomy S.S. Mikhailov, A.V. Chukbar, A.G. Tsybulkin
A person who wants to take full care of his health oral cavity must know the structure of the tooth and the easiest way to do this is according to diagrams where there is detailed description each layer. This will allow you to be confident when visiting the dentist and not be afraid of previously incomprehensible definitions.
In addition, the anatomy of the teeth of the upper and lower jaws will give any person basic information about the pain that occurs. For example on early stages caries, a person feels discomfort due to irritants (cold, hot, sweet), and when he gets to the pulp, painful sensations intensify so much that they cannot be tolerated.
It should also be noted that in adults, molars, unlike baby teeth in children, will not grow back later and they will have to be restored using filling materials and dental structures, depending on the damage caused.
Features of the anatomical structure
Despite the hardness and integrity of some elements, they consist of several layers and the same applies to teeth, and private anatomy can tell about their structure and functions of individual parts.
Tooth structure:
This is anatomical structure human teeth located on the upper and lower jaws and without pathologies, they perform all their functions correctly and without causing discomfort.
Histology
Histology can tell you about the cross-sectional structure of a human tooth, as well as its structure. She will describe each layer, as well as its functions, which will be very useful for people who want to learn more about their body.
Teeth structure:
The tooth is supported by a combination of soft tissues that form the periodontal ligament system.
The structure of the tooth also includes the apical foramen, located at the very top of the root. Nerves come out of him and blood vessels, which further connect with nerve fibers and the rest circulatory system body.
Types and functions of teeth
 After it has become clear what a person’s teeth are made of, it is necessary to find out what types they have and what functions they perform. This will answer many questions related to grinding food, for example, which teeth are chewing teeth, and what makes it possible to bite off pieces of food.
After it has become clear what a person’s teeth are made of, it is necessary to find out what types they have and what functions they perform. This will answer many questions related to grinding food, for example, which teeth are chewing teeth, and what makes it possible to bite off pieces of food.
Adults, unlike children, have 32 teeth in their mouths, respectively 16 on each jaw and therefore 8 on each side. At the same time, you need to understand that not every person has 8 (3rd molar) and therefore it is quite normal if they total quantity will be 28. In order to understand how they are located in dentistry, they introduced special ones, where the teeth are numbered from 1 to 8, namely:
- Under the numbers 1 and 2 there are incisors on both sides;
- Under the number 3 are the fangs;
- The numbers 4 and 5 were given to the premolars;
- The molars were numbered from 6 to 8.
The teeth should be located symmetrically above each other, for example, the canine of the upper jaw should be above the lower one and cover it by one third, and the same applies to the incisors, premolars and molars.
In addition, in order to understand how a tooth is structured, you need to remember what forms it is divided into and what functions they perform, and for this you can focus on the following description:
- Incisors. They are flat in shape and designed for biting off pieces of food. It is worth noting that the upper incisors are larger in size than the lower ones;
- Fangs. Since ancient times, they have become less sharp, but still retain their cone-shaped profile. The fangs serve to firmly grasp the food and then, with the help of the incisors, bite off a piece;
- Premolars. They follow each other and their function is to chew food. In addition, premolars provide aesthetic appearance cheekbones, due to its angular position;
- Molars. They are 3 outer teeth going one after the other, but if there are no 8, then there are only 2 of them on each side of both jaws. Molars, like premolars, are used for chewing food, but they are larger. In addition, they, unlike the listed types of teeth, have 2 root processes, and 3 on the upper jaw;
- Wisdom tooth (3rd molar). It is considered to be closing on both jaws. Dentists call it a rudiment, which to modern man is not needed and often such a tooth appears with defects. The process of teething can begin either at the age of 15-17 or at 27, and it is better to go to the hospital to have it done X-ray and understand when you can expect it.
Baby teeth
 Milk teeth in children, unlike permanent teeth, have their own slight differences in structure. It should also be noted that no more than 20 of them will appear and the last one will thin out by about 3 years.
Milk teeth in children, unlike permanent teeth, have their own slight differences in structure. It should also be noted that no more than 20 of them will appear and the last one will thin out by about 3 years.
Differences between temporary teeth in children and permanent teeth:
- The crown of baby teeth is much smaller;
- The enamel is represented by a thinner layer. In addition, dentin is not so mineralized and therefore baby teeth are easily susceptible to caries;
- The pulp capsule and root canals in baby teeth have a larger volume than in permanent teeth and therefore inflammatory processes occur more often in them;
- The tubercles, which are located on the chewing and cutting surfaces, do not stand out much in comparison with permanent teeth;
- In children, the primary incisors are more convex;
- Their root system is much less developed, so permanent teeth replace them without any problems, and children do not feel much discomfort.
The structure of the tooth is important knowledge that will be useful to any person who wants to preserve healthy smile. In addition, this will make it possible to understand complicated dental terms and help more accurately localize the discomfort that appears in the mouth.
Human teeth begin to form at the stage intrauterine development(7-8 weeks). Part of the epithelium thickens, then a curved fold with its edges grows deep into the surrounding tissue, forming a dental plate (1). The fold itself is uneven, usually clusters of cells (dental papillae) are formed, above them something like bells protruding upward is obtained. Subsequently, enamel is formed from this epithelium itself (2), and dentin and pulp are formed from the tissues inside the bell (3). This same tissue supplies stem cells for the growing tooth. Large folds (2,3), laid down very first, become the rudiments of milk teeth. At the 5th month of pregnancy, the rudiments begin to develop from smaller bell-shaped folds (4). permanent teeth.



This process itself determines the further structure of the tooth: since the protein matrix of the enamel is formed only from the area of the ingrown epidermis, the shape of the crown and the thickness of the tooth enamel in an adult strongly depends on the characteristics of its intrauterine development at the end of the second month of pregnancy. An epidermal plate that is not deeply ingrown or receives insufficient nutrition will give rise to a small crown, or a crown with an enamel defect or with thin enamel. At this same stage, the number of teeth is formed, and the rudiments of both milk and permanent teeth are immediately formed. Normally, a person has 20 primary teeth and 28-32 permanent teeth, but there may be more or fewer teeth: this depends on the number of markers and signal sources.
The roots of the tooth are formed before eruption, and the final shape is taken 6-8 months after it (sometimes later).


Sometimes third molars do not grow at all, sometimes they grow inside the jaw, causing problems.

After the eruption of permanent molars, dental plasticity disappears, and new teeth can no longer appear. However, if “extra” rudiments remain in the jaw, they can sometimes be activated. The shape and arrangement of teeth are unique to each person. According to some studies, early human ancestors had 44 teeth, so sometimes atavisms occur regarding the increase in the dentition: either additional teeth in the main arches, or additional teeth on the palate.
Important! The formation of teeth depends on the characteristics of pregnancy. Maternal malnutrition, vitamin deficiencies (especially lack of vitamin D) or the use of antibiotics can lead to dental hypoplasia in the newborn, and both milk and permanent teeth can be damaged.
Dental formulas
In humans different teeth have different functions, and are of four types in shape. To describe the location of teeth, there are so-called dental formulas. Dental formula a person has 32 teeth.

IN simple version dental formulas simply indicate the tooth number (No. 1 central incisor), in the second case they add a number that indicates on which jaw and side the tooth is located.

The dental formula for primary occlusion is written in Roman numerals or designated as numbers 5-8.

Anatomical structure of the tooth
In a tooth, there is a crown (protrudes above the gum, covered with enamel), a root (located in the jaw socket, covered with cement) and a neck - the place where the enamel ends and cement begins; such a neck is called “anatomical”. Normally, it should be slightly below the level of the gum. In addition, a “clinical neck” is distinguished, this is the level of the dental-gingival groove. The neck looks like a narrowed part of the tooth; above and below it it usually widens.

Normally, the clinical neck is higher than the anatomical one, and the gum border runs along the enamel. However, with age, the gums atrophy and the enamel is destroyed. At certain times, it may happen that the clinical and anatomical necks coincide. In old age, when the gums descend lower and the enamel becomes thinner, wears out and disappears (near the neck it is thinner and disappears earlier), a gap appears again between these conventional boundaries, but now the level of the clinical neck will pass along the exposed dentin of the tooth.

The crown of the incisors is chisel-shaped, slightly curved, with three cutting cusps; in fangs - flattened-conical; in premolars it is prismatic or cubic, with rounded sides, with 2 chewing cusps; molars (molars) are rectangular or cubic in shape with 3-5 chewing cusps.

The tubercles are separated by grooves - fissures. Incisors, canines and second premolars have one root, first premolars have a double root, and molars have a triple root. However, sometimes molars can have 4-5 roots, and the roots and canals in them can be curved in the most strange way. That is why tooth depulpation and canal filling are always done under X-ray control: the dentist must make sure that he has found and filled all the canals.

The tooth is secured in the alveolar socket using strong collagen strands. The cementum covering the root is made of collagen impregnated with mineral salts, and the periodontium is attached to it. The tooth is nourished and innervated by the arteries, veins and processes of the trigeminal nerve entering the opening of the root apex.
The length of the root is usually twice the length of the crown.

Histological structure of the tooth
The tooth consists of three types of calcified tissue: enamel, dentin, cement. Enamel is the strongest, dentin is 5-10 times weaker than it, but 5-10 times stronger than ordinary bone tissue. Both dentin and enamel are a protein mesh-fibrous matrix impregnated with calcium salts, although dentin in structure is between enamel and dense bone tissue. If crystals of mineral salts (apatites) are lost, the strength of the tooth can be restored, since salt crystals, under favorable conditions, will again be deposited on the protein frame; however, if part of the protein matrix of the enamel is lost (for example, by chipping, drilling or grinding), this loss is irreplaceable for the tooth.
The thickness of the enamel on the lateral surfaces of the crown is 1-1.3 mm, on the cutting edge and chewing cusps up to 3.5 mm. The tooth erupts with non-mineralized enamel, at which time it is covered with a cuticle. Over time, it wears out and is replaced by the pellicle, and further mineralization of the pellicle and enamel occurs in the oral cavity due to the salts contained in saliva and dental-gingival fluid.
There are no cells inside dentin; it can partially become compacted and loosened; a protein matrix can grow in it, but only in a chamber limited by the inner surface of the enamel. Nevertheless, age-related demineralization predominates in humans. Dentin consists of thin calcified tubes running radially from the enamel to the pulp. If foreign substances or liquid enter these tubes, increased internal pressure transmitted to the pulp, causing pain (the greater the pressure inside the dentinal tubule).

Pulp is loose connective tissue. It is penetrated by nerves, lymphatic and blood vessels and fills the pulp chamber of the crown and root, and the shape of the chamber can be any. The larger the pulp relative to the overall size of the tooth, the weaker and more sensitive it is to temperatures and chemicals.
Functions of the pulp:
- transmits sensory information to the brain;
- nourishes living tooth tissues;
- participates in the processes of mineralization and demineralization;
- its cells synthesize proteins that are integrated into the protein matrix of the tooth.
The structure of baby teeth
A child is born with practically formed primordia of baby teeth. They begin to erupt already at 3-4 months of life and already at this time require care. By the time teeth erupt, the roots have not yet been fully formed, since the root grows for quite a long time. The rudiments of permanent teeth also continue to develop in the jaw, their crowns grow, but the roots will begin to form only by the time the teeth change.
In baby teeth, the tops of the roots are bent to the buccal side, and between their roots there are the rudiments of permanent teeth.

Milk teeth have a weaker layer of dentin and less mineralized enamel, their roots are shorter and thicker than those of permanent teeth of the same name. The cutting edge of the incisors usually has slightly pronounced tubercles, and the chewing tubercles are also insignificant. A large volume of pulp and a thin layer of dentin make such teeth more sensitive to sour, sweet, and hot foods. Since they are less mineralized, they are more susceptible to caries and pulpitis, and local anesthetics during treatment inhibit the production of stem cells and dentin growth in the rudiments of permanent teeth.
Important: caries that begins in baby teeth is easily transmitted to the permanent ones that replace them, since the bacteria that cause it continue to develop in the oral cavity. A baby usually gets these bacteria from the mother if she feeds him with the same spoon she eats with, or licks a fallen pacifier (instead of washing it).
Replacing teeth with permanent ones
By the time the teeth change and the active growth of the branches of the jaw begins, the child has 20 teeth. At this time, there are 2 molars on each side, but no premolars. It is the premolars that will take up the free space that appears in the branches growing in length. If the jaw does not grow quickly enough, a defect in the dentition may appear.

When changing teeth, the growing germ of a permanent tooth compresses the roots of the milk teeth, pinching the blood vessels that feed them. Gradually, the roots of baby teeth, lacking nutrition, begin to collapse and completely dissolve, so that only the neck of the tooth and the crown remain. However, the rudiments of permanent ones may also suffer. Sometimes they are involved in the process and are completely destroyed, sometimes enamel defects occur, since its protein-collagen matrix, formed from the epithelium, can easily be damaged at this stage. Hypoplasia (underdevelopment) of the tooth and the eruption of teeth with damaged enamel are very common in recent years.

Anomalies of teeth and dentition
Anomalies of tooth structure
- too large (more than five) number of roots;
- root underdevelopment;
- uncharacteristic shape (subulate, hook-shaped, conical, flat crowns);
- underdeveloped, deformed crown;
- thin enamel;
- increased abrasion of enamel;
- absence of all or part of the enamel.
Anomalies of changing teeth
- the root may not resolve in time;
- the tip of the root can pierce the bone, causing an ulcer in the gum;
- the root is completely exposed, as all the tissue (both bone and gums) above it is destroyed;
- permanent tooth started to grow before the milk fell out;
- an additional row of permanent teeth or teeth in the roof of the mouth is formed;
- There is not enough space for normal tooth growth.

Anomalies of the dentition
- malocclusion;
- anomalies in the location of teeth in the dentition.
In all cases of anomalies with root resorption, baby teeth must be removed. If teeth grow in two or three rows or are crooked, extraction of baby teeth may also be indicated. At the same time, removing a tooth too early (for example, due to caries) can cause permanent teeth to start growing earlier, or cause the growth of additional teeth (usually small, conical ones). Additional teeth corresponding in shape to molars are formed less frequently.
0A person's teeth change only once. The teeth of the mixed bite are called temporary. Their eruption begins at the 6-7th month of life and ends at 2.5-3 years. At 5-6 years of age, teeth begin to erupt permanent dentition(dentes permanenetes), and by the age of 13, temporary teeth are completely replaced by permanent teeth. The number of temporary and permanent teeth is not the same: in the temporary dentition there are only 20 teeth, since premolars and third molars are missing. The anatomical formula of the teeth of the temporary occlusion is 2.1.1, i.e. on each side of both the upper and lower jaws there are 2 incisors, 1 canine and 2 molars.
There are 32 teeth in the permanent dentition. Their anatomical formula is 2.1.2.3, i.e. 2 incisors, 1 canine, 2 premolars and 3 molars.
In teeth of temporary and permanent bite, a crown (corona dentis) is distinguished - the part of the tooth protruding into the oral cavity; the root of the tooth (radix dentis), which is located in the alveolus; neck of the tooth (cervix dentis) - a slight narrowing at the border between the crown and root of the tooth. At the level of the neck of the tooth, the enamel cover of the crown ends and the cement covering the root of the tooth begins. In the area of the neck of the tooth, the circular ligament is attached, the fibers of which on the opposite side are woven into the bone of the alveoli, gum, and are also directed to the necks of neighboring teeth (Fig. 3.5).
Rice. 3.5. Tooth structure (diagram): 1 - crown; 2 - root; 3 - neck; 4 - enamel; 5 - dentin; 6 - pulp: 7 - gums; 8 - periodontium; 9 - bone alveolar process.
Inside the tooth there is a tooth cavity (cavitas dentis), which is divided into the coronal part (cavitas coronale) and the casal of the tooth root, or root canal (canalis radicis dentis), in the apex area the root ends with a narrow apical (apical) opening (foramen apices dentis).
The following surfaces are distinguished on the crown of teeth: mesial (mesial surface), cystal (distal surface), facial, or vestibular (facial surface), lingual (lingual surface). Premolars and molars also have an occlusal (chewing) surface. The line of convergence of the lingual and facial surfaces of the incisors and canines forms the cutting edge.
Each tooth has anatomical features, allowing one to determine its group affiliation. Such signs are the shape of the crown, cutting edge or chewing surface, and the number of roots. Along with this, there are signs that the tooth belongs to the right or left jaw: signs of crown curvature, crown angle, root sign.
A sign of crown curvature is manifested in the fact that the greatest convexity of the vestibular (dental, cheek) surface is located mesially (Fig. 3.6, a). The sign of the crown angle is expressed in the fact that the mesial surface and the cutting edge of the incisors and canines form more
The completion of teething (temporary and permanent) ends with the formation of dentition in the form of arches. The upper row of permanent teeth has the shape of a semi-ellipse, the lower one - a parabola (Fig. 3.7). In this case, the upper dentition is wider than the lower one, as a result of which the upper incisors and canines overlap the teeth of the same name, and the buccal cusps of the upper chewing teeth are located outward from the lower ones of the same name.
The dentition is functionally a single whole, which is due to a number of factors. It is known that the crown of the tooth has a convexity, especially pronounced in premolars and molars. It is called the equator of the tooth and is located on the border of the upper and middle third of the crown. The presence of convexity ensures the creation of interdental contacts, which in incisors and canines are located closer to the cutting edge than in premolars and molars. As a result, a triangular space is created between the teeth, filled with a gingival papilla, which is thus protected from food. In addition, the presence of tight contact between the teeth ensures the unity of the dentition, which creates high functional stability when chewing. The pressure exerted on any tooth extends not only along its roots to the alveolar process, but also to adjacent teeth thanks to their close contact. With age, point contact points turn into planar ones, which is explained by the physiological mobility of teeth. Creation, or rather restoration, of a dense contact point during restoration is prerequisite guaranteed treatment.
The location of the teeth in the alveolar process plays a significant role in the stability of the dentition. Thus, the teeth of the lower jaw are inclined with their crowns inward and their roots outward. In addition, the crowns of the lower molars are inclined forward. The convexity of the dental arch, combined with the tight contact and internal inclination of the crown, ensures reliable fixation of the lower jaw teeth.
The inclination of the teeth of the upper jaw contributes less to their stability, since their crowns are inclined outward
According to available data, the angle of inclination of the crowns of the maxillary molars in the facial (vestibular)-distal direction reaches 10-20°, and of the crowns of the lower jaw in the mesial-lingual direction - 10-25°. The angle of inclination of the tooth crown should be taken into account during trephination during endodontic treatment to avoid perforation.
The incisors and canines of the upper and lower jaws have a significant inclination of the crowns, which should also be remembered when opening and processing the tooth cavity.
The maxillary central incisors are the largest of the group of incisors. Their vestibular surface is convex. There are two faint grooves on it, running from the central part of the crown to the cutting edge. The lingual surface has triangular shape, concave. The side surfaces also have the shape of a triangle. The root is powerful, cone-shaped. There is a longitudinal depression (groove) on the mesial surface of the root. Signs of crown and angle curvature are well expressed. The average tooth length is 25 mm (23.5-25.5). It has 1 root and 1 channel 100% of the time.
The lateral incisors of the upper jaw (see Fig. 3.10) are smaller in size than the central ones. The mesial surface meets the cutting edge at a right angle, the lateral angle is rounded. The lingual surface is concave. Pronounced lateral ridges, when converging at the neck of the tooth, form a fossa. The root is compressed from the sides, the lateral groove is clearly visible. The distal bend of the root is pronounced. The channel has an oval shape. The average tooth length is 23 mm (21-25 mm). It has 1 root and 1 channel 100% of the time.
The central incisors of the lower jaw are significantly smaller than the incisors of the upper jaw (see Fig. 3.10). Their average length is 21 mm (19-23). (L. 1 root and 1 canal are found in 70% of cases, 1 root and 2 canals - in 30%, but in most cases they end in one hole. The canals are located in the lingual-vestibular direction. For this reason, on the radiograph the second canal is almost always not detected.
The lateral incisors of the lower jaw are somewhat larger than the central ones (see Fig. 3.10). The average size 22 mm (20-24). In 67% of cases there is 1 root and 1 canal, in 40% - 2 roots and 2 canals, in 13% - 2 roots converging at the apex. The root is well developed, conical different shapes, compressed laterally. The channels are narrow.
The canines of the upper jaw (Fig. 3.11) are the longest teeth, averaging 27 mm (24-29.7 mm). Always have 1 root and 1 channel. The tooth cavity is of significant size, oval in shape with expansion in the vestibular-lingual direction at the level of the neck. The cutting edge of the canine is formed by two segments converging at an angle, of which the mesial one is shorter than the lateral one. The vestibular and lingual surfaces are convex, the contact surfaces are triangular in shape. The root is powerful, slightly compressed from the sides. The root tip is often curved.
The canines of the lower jaw (see Fig. 3.11) are somewhat smaller than the canines of the upper jaw. Their average length is 26 mm (26.5-28.5). 1 root and 1 canal are detected in 94%, 2 canals - in 6%. The canal is oval in shape and passable well.
First premolars of the maxilla (Fig. 3.12). The shape of the crown resembles a rounded rectangle. The chewing surface is formed by two tubercles - vestibular and lingual, of which the lingual one is smaller than the vestibular one. The fissure separating the cusps ends in a small depression, which is limited by an enamel ridge at the site of the transition of the masticatory to the mesial and distal surfaces of the crown. The average tooth length is 21 mm (19-23 mm). Has 2 roots and 2 canals in 79% of cases; 1 root and 1 channel - 18%; 3 roots and 3 canals - in 3% of cases.
The second premolars of the upper jaw (see Fig. 3.12) are almost the same in shape as the first, but are smaller in size. The chewing surface has two tubercles of the same size. The root is usually single and slightly flattened. There is a tendency for the root to bifurcate. The average tooth length is 22 mm (20-24 mm). In 56% it has 1 root and 1 canal, in 42% - 2 roots and 2 canals; in 2% - 3 roots and 3 channels. The tooth cavity is located at the level of the neck.
First premolars of the mandible (see Fig. 3.12). Their average length is 22 mm (20-24). They have 1 root and 1 canal in 74%, or 1 root and 2 canals converging at the apex - in 26%. Round crown, chewing surface formed by 2 tubercles, of which the buccal one is much larger than the lingual one, which imparts an inclination of the tooth crown into the oral cavity. The cusps are separated by a small groove, which is always located closer to the lingual cusp. At the anterior and posterior surfaces, the tubercles are connected by enamel ridges. In other cases, an enamel ridge runs from the middle of the buccal cusp to the lingual one, and then two pits form on its sides on the chewing surface. The buccal surface is convex, the sign of curvature is well expressed, the contact surfaces are also convex and gradually transform into the lingual surface. The root is oval in shape, with faint grooves on the front and back surfaces. Often the crown and root are located at an angle to each other with an inclination towards the tongue. The root sign is well expressed.
The second premolars of the lower jaw (in size exceed the first premolars of the same jaw.
Their average length is 22 mm (20-24). In 97% of cases they have 1 root and 1 canal, in 3% - 1 root and 2 canals. The chewing surface consists of two almost equally developed tubercles, which are connected in the center by an enamel ridge. There is a deep groove between the hillocks; often an additional groove extends from it, which divides the lingual cusp into two, turning the tooth into a tricuspid one. The buccal surface is the same as that of the first premolar, the contact surfaces are slightly bigger size and convex. Thanks to the well-developed buccal cusp, the chewing surface is inclined towards the oral cavity. The root is cone-shaped and more developed in comparison with the first premolar. The coronal part of the tooth cavity is compressed in the anteroposterior direction and has the shape of a gap with two protrusions corresponding to the cusps of the crown.
The first molars of the maxilla are the largest teeth. Average length 22 mm (20-24 mm). The chewing surface of the tooth has the shape of a rounded diamond and is formed by 4 tubercles separated by fissures. One of the fissures, starting on the front surface, crosses the chewing surface and goes to the buccal surface, where it continues to the middle of the crown. This groove separates the anterior buccal cusp. The second groove begins on the posterior surface, passes to the chewing, and then to the lingual, separating the posterior lingual tubercle. The third fissure connects the first two, defining the remaining tubercles. On the anterior lingual tubercle there is usually an anomalous (additional) tubercle (tuberculum anomale Carabelli), which never reaches the chewing surface.
2 canals are located in the mesial buccal root, which has a flattened shape. In 3% of cases there are 5 roots - an additional root is identified in the distal buccal root.
The tooth cavity is shifted to the anterior third of the crown, and the mouths of the canals are located at an obtuse angle. The mouth of the fourth canal is located along the line of connection between the mouth of the buccal and palatal canals at a distance of 1.5-2 mm from the buccal canal.
Maxillary second molars (see Fig. 3.13). The average tooth length is 21 mm (19-23). The shape of the crown, like the shape of the chewing surface, has four options - two options with 4 cusps and two with 3 cusps. In the first option, the shape of the crown and chewing surface is the same as in the first molar. The difference is the absence of an additional tubercle. This variant occurs in 45% of Europeans.
The second option is that the crown is elongated in the mesial-distal direction and resembles an elongated prism with well-defined 4 cusps. The mesiobuccal and distal-lingual fissures are well defined and the intermediate fissures are poorly defined.
The third option is that the crown is also elongated in length, but there are 3 well-defined tubercles located in a straight line and separated by fissures.
The fourth option - the crown, like the chewing surface, has a triangular shape formed by three tubercles: 1 lingual, 2 buccal. The variant occurs in approximately 52% of cases. As a rule, a tooth has 3 roots and 3 canals (65%), 3 roots and 4 canals (35%).
The third molars of the upper jaw (see Fig. 3.13) are characterized by variable shape and size, but are often smaller. The crown usually has 3 tubercles, somewhat less often - 4, but there may be 5-6 tubercles. The size and shape of tooth roots are also variable; their number can vary from 1 to 4-5.
First molars of the mandible (see Fig. 3.13). Their average length is 22 mm (20-24). They usually have 2 roots and 3 canals (2 in the mesial root, 1 in the distal) - in 65%. In 29% of cases, 4 canals are found (2 in the mesial and 2 in the distal), in 6% - 2 canals. The chewing surface is formed by 5 tubercles due to two intersecting fissures running in the mesial-distal and buccal-lingual directions and an additional groove in the posterior buccal area of the chewing surface. This arrangement of grooves forms 5 tubercles on the chewing surface: 3 buccal and 2 lingual. The buccal surface is convex, with a well-defined sign of crown curvature. The tooth cavity is of considerable size and slightly shifted in the mesial-buccal direction. There are 2 canals in the mesial root: buccal, located in the mesial-buccal direction, and lingual, located at a distance of 2-3 mm from it. If there are 4 canals instead of 1 distal, there are 2 - buccal and lingual. In this case, the tooth cavity has the shape of a pronounced rectangle with rounded corners.
The second molars of the mandible are somewhat smaller than the first. The shape of the chewing surface is determined by two fissures. One of them runs in the mesial-distal direction, separating the buccal and lingual cusps. The fissures end in depressions, which are limited by enamel ridges at the transition point of the chewing surface to the mesial and distal. The second fissure runs in the lingual-buccal direction and, in most cases, reaches the blind fossa in the middle of the buccal surface. The teeth have 2 roots - mesial and distal and 3 canals - 1 distal and 2 mesial. It is important to remember that the mouth of the buccal-mesial canal is displaced in the buccal direction. In 28% of cases there may be 4 canals, in 8% there may be a fusion of the mesial and distal canals.
Mandibular third molars can be of different shapes. More often, the chewing surface consists of 4 tubercles, but 5-tubercle teeth are also often found. There have been cases where a tooth had 6-7 cusps. In most cases, there are 2 roots, but often they merge into one cone-shaped one. Occasionally there are several underdeveloped roots. The cavity of the tooth follows its shape, but the size and shape of the roots are not constant.
In conclusion, it is necessary to dwell on anatomical formations who play important role For clinical practice. First of all, you should pay attention to the presence of the tooth equator (spherical surface) on the cheek and contact surfaces, which is necessary to prevent gum injury during chewing food. In the process of considering the structure of the crown of premolars and molars, the existence of an enamel ridge on the chewing surface, at the border of its transition to the mesial or distal, was mentioned. Its significance is due to the fact that it prevents food from entering the interdental space. In the event that a cushion is not formed during the formation of the chewing surface, but a flat surface is created, which is most often observed during filling, then food enters the interdental space, despite the presence of a contact point
And the last thing is the condition of the fissures of the chewing surface. Fissures are distinguished by depth (superficial and deep) and by shape - open, V-shaped and ampoule-shaped. In the presence of deep fissures with an ampoule-shaped expansion, preventive preparation is indicated.
- Histological and anatomical structure
- Types of teeth and their differences
- Structure in children
- Numbering is an important component for a dentist
Knowing the structure of teeth, a person will be able to properly care for them and better understand the dentist’s recommendations. Teeth are not able to recover after destruction, so they must be protected. If someone thinks they are quite hard, then this is not entirely true - without some care, the hardness will be apparent.
Histological and anatomical structure
Human teeth perform different functions and, accordingly, differ in shape from each other. But on internal structure they are all similar. A more clear idea of what a tooth consists of will be given by a diagram of its structure (IMAGE 1).
The tooth consists of the following tissues:

Image 1. Diagram of the tooth structure.
- Enamel. This is the most hard fabric in the human body. It covers each tooth from the outside. In addition to hardness, it is also very durable (in this parameter it is only slightly inferior to diamond). Enamel consists of at least 95% calcium mineral salts. The rest is water, but there is very little of it in this fabric. Lipid and protein compounds are also present in the enamel, but their volume is minimal.
- The next layer, located immediately under the enamel, dentin is the base of the tooth. This is also a fairly hard tissue, consisting of 70% inorganic elements. In structure, dentin is close to bones, but is stronger because it is mineralized. It surrounds the hollow part of the tooth and the root canal. Microscopically sized canals extend towards dentin from the central dental tissues. They are necessary for metabolic processes, including the exchange of nerve impulses.
- Dentin is followed by pulp. This is connective tissue, soft in structure. It is penetrated by vessels, blood and lymphatic, and nerves. They are all divided into branches that go to a specific root. The pulp plays an important role - through it the nutrition of the tooth is provided and metabolism occurs. Once the pulp is removed, everything metabolic processes stop.
The anatomical structure of the tooth is as follows:
- crown - the part that is visible to the naked eye (it is located above the gum);
- neck - the place where the root and crown connect;
- root - the inner part (that which is not visible).
The crown has 4 surfaces - closure (with the second jaw), facial (from the cheeks), lingual (with inside), contact (in the vicinity of nearby teeth).
The neck is a slightly narrowed tooth part. It is surrounded by connective fibers responsible for the ligament of the tooth.
The root is deepened in the gum. The location of the depression is the alveolus. At the end of the root there is an opening through which the vessels responsible for feeding the tooth and nerves pass.
Between the root and the alveolus there is a space called the periodontium.
Return to contents
Types of teeth and their differences
Upper or lower jaw has 4 types of teeth: incisor, canine, premolar and molar. Each type has its own purpose and individual shape.
The jaw is divided into 2 symmetrical halves. On each of them, the teeth are arranged as follows: two incisors, one canine, two premolars and three molars. In the second half the arrangement is exactly the same. Moreover, the 3rd molar is . They grow later than others - when a person has already matured. Some people don't have them at all. As a result, there are 16 teeth on each human jaw (if there is no 3rd molar, then 14). There are 32 (or 28) teeth in a person’s mouth.
The incisors are located in the center of the jaw. They have another name - anterior (frontal). The incisor has a single root. Its crown is flat, and its edge has a cutting appearance. It is convex in front and concave in back. The crown of the upper jaw is large, and the lower one is small. The incisors are only responsible for biting food. They are not able to chew food, as they are the weakest teeth, unable to withstand significant loads. But they are best at biting food because of their structure.
 The canines are located in the corners of the dental arches. There are 4 of them in total - 2 on each jaw. Their task is to tear off those pieces of food that the incisors cannot handle. The fang has a powerful crown. It has a single root, but longer and much more powerful than that of the incisor. Due to their favorable location, thanks to the strong root and crown, the canines are the most stable in the entire dentition.
The canines are located in the corners of the dental arches. There are 4 of them in total - 2 on each jaw. Their task is to tear off those pieces of food that the incisors cannot handle. The fang has a powerful crown. It has a single root, but longer and much more powerful than that of the incisor. Due to their favorable location, thanks to the strong root and crown, the canines are the most stable in the entire dentition.
Premolars are the smallest in the dentition. Their place is directly behind the fangs. They are designed for capturing and chewing food. In premolars, the crown has a wide surface, so the tooth does not experience stress from this function. Premolars have a single root, only the first one on the upper jaw has two. There are no teeth of this type among milk teeth.
The largest teeth in the dentition are molars. Their purpose is to grind food and grind it. For this you need significant effort, which is ensured by the large surface of the crown. The upper molars have 3 roots, and the lower molars have 2.
They are different in size. The first of the three is the largest, then they decrease in size. Both the chewing surface and the length of the root decrease.
Some people have jaw abnormalities—some types of teeth may be missing.
Return to contents
Structure in children
 Children's teeth are very important for the development of future permanent teeth. It is wrong to think that you don’t have to take care of your baby teeth. If a child loses an incisor prematurely, this is fraught with consequences - the permanent tooth may be of irregular shape or grow in the wrong place where it should be. The deciduous incisors also play a role in bite.
Children's teeth are very important for the development of future permanent teeth. It is wrong to think that you don’t have to take care of your baby teeth. If a child loses an incisor prematurely, this is fraught with consequences - the permanent tooth may be of irregular shape or grow in the wrong place where it should be. The deciduous incisors also play a role in bite.
The structure of baby teeth is different from permanent teeth - they are much less protected. Their enamel and dentin are too thin. This contributes to the significant development of caries. Through thin enamel, various harmful microorganisms easily enter the pulp. It is too voluminous, with a large number of channels, which also helps bacteria penetrate inside the tooth. Therefore, it is necessary to brush your teeth from a very young age. Primary teeth have much smaller crowns than permanent teeth, and their roots are wider.
The anatomical structure of teeth in children contributes to the development various diseases oral cavity. This is both caries and malocclusion, and periostitis. Parents must understand that their child needs to be taken to see doctors more often. pediatric dentist. Milk teeth are guides for permanent teeth.
Children's incisors show a permanent path for development and growth, including determining the place where the main tooth will subsequently be located.
Therefore, they need to be monitored and treated promptly if necessary.
")